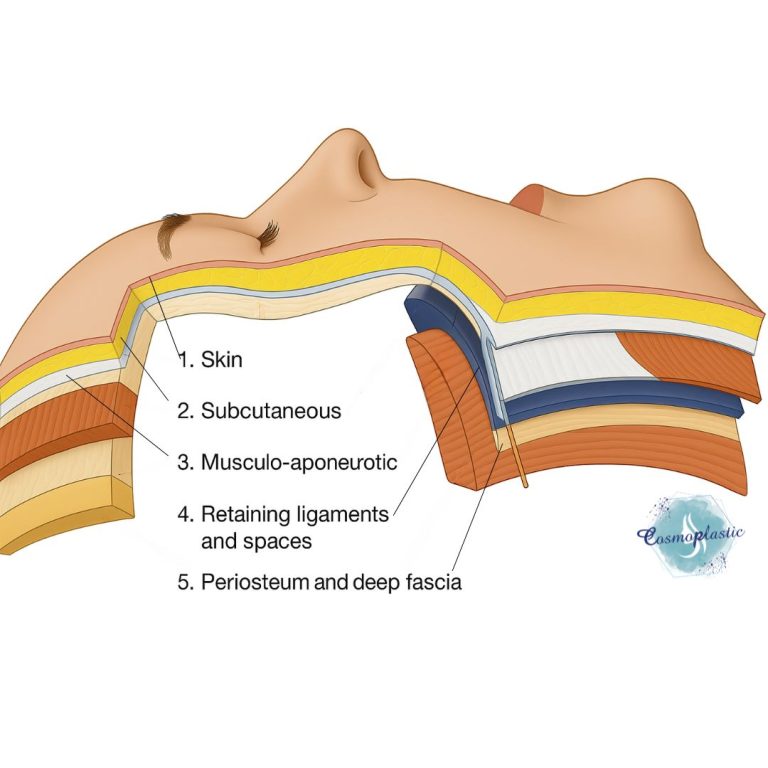
The SMAS is a continuous, fibromuscular layer:
- It is situated deep to the subcutaneous fat and superficial to the mimetic muscles and deeper fascial layers.
- It is composed of fibrous tissue interwoven with muscle fibers and acts as a conduit for facial expression.
Anatomical Extension & Regional Relations
A. Temporal Region
The SMAS continues superiorly as the temporal parietal fascia.
Superficial to the deep temporal fascia (which covers the temporalis muscle).
It is continuous with the galea aponeurotica of the scalp (epicranial aponeurosis).
The superficial temporal fat pad lies just under this layer.
B. Cheek and Midface
Over the zygomaticus major and minor, the SMAS envelops these muscles, forming mobile fascial planes.
The SMAS is tightly adherent to the malar septum and sends fibrous septa to the dermis, aiding midface contour.
Extends medially towards the nasolabial fold, where it becomes thinner and fuses with mimetic muscles.
C. Parotid Region
SMAS overlies the parotidomasseteric fascia, which itself covers the parotid gland and masseter muscle.
The facial nerve branches travel deep to the SMAS and within or beneath the parotidomasseteric fascia.
This zone is critical during facelifts to avoid nerve injury.
D. Lower Face and Mandibular Border
SMAS continues inferiorly to blend with the platysma muscle in the lower face and neck.
Forms ligamentous attachments to the mandibular border via mandibular retaining ligaments, e.g., mandibular septum and marginal mandibular ligament.
E. Neck
The platysma muscle is the cervical extension of the SMAS.
It is continuous from the superficial cervical fascia and contributes to neck contour and movement.
Areas with Different Extensions or Absent SMAS
Certain facial regions lack a true SMAS and instead exhibit analogous or distinct structures:
A. Central Midface (Nasal Region)
SMAS becomes ill-defined over the nose.
Over the nasal dorsum and alae, the SMAS is replaced by fibroareolar tissue directly connected to the nasalis muscle.
This region is less mobile and not targeted in traditional facelifts.
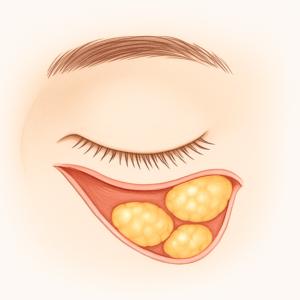
B. Upper and Lower Eyelids
The SMAS terminates superior to the orbit at the orbicularis retaining ligament.
In the eyelids:
- The orbicularis oculi muscle lies directly beneath the skin and subcutaneous tissue
- No true SMAS exists; instead, there is a thin orbital septum and preseptal fascia.
- This makes eyelid dissection delicate and not amenable to deep plane SMAS lifting.
C. Perioral Region
Overlying the modiolus and orbicularis oris, the SMAS thins significantly or becomes discontinuous.
This area relies more on dense muscular and fibrous interconnections than a distinct fascial layer.
Surgical Relevance
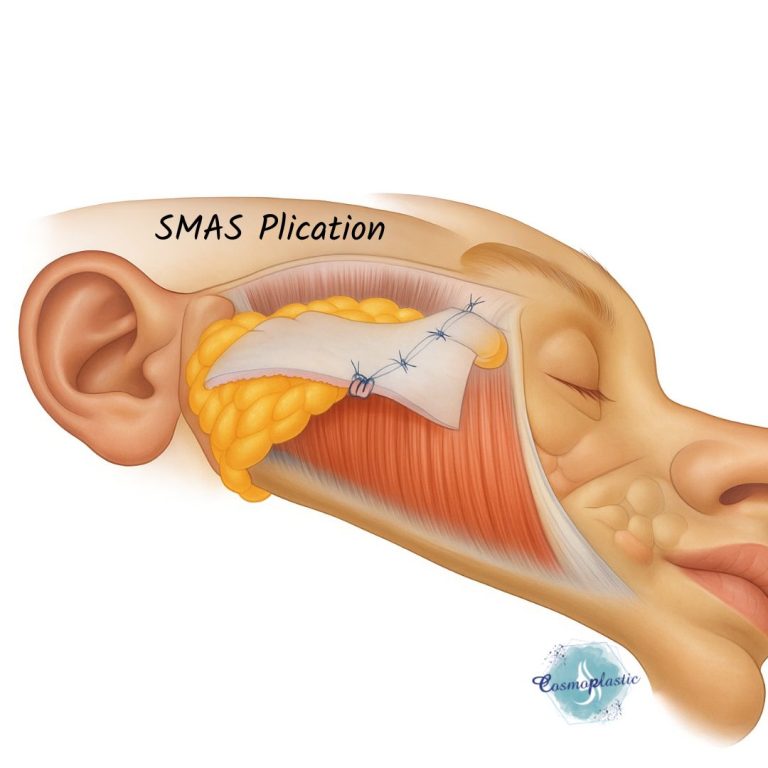
● Facelift Surgery: The SMAS layer is a key target in rhytidectomy. Surgical manipulation, such as plication or SMASectomy, enhances midface elevation and skin redraping while minimizing tension on the skin, reducing scar risks and improving longevity of results.
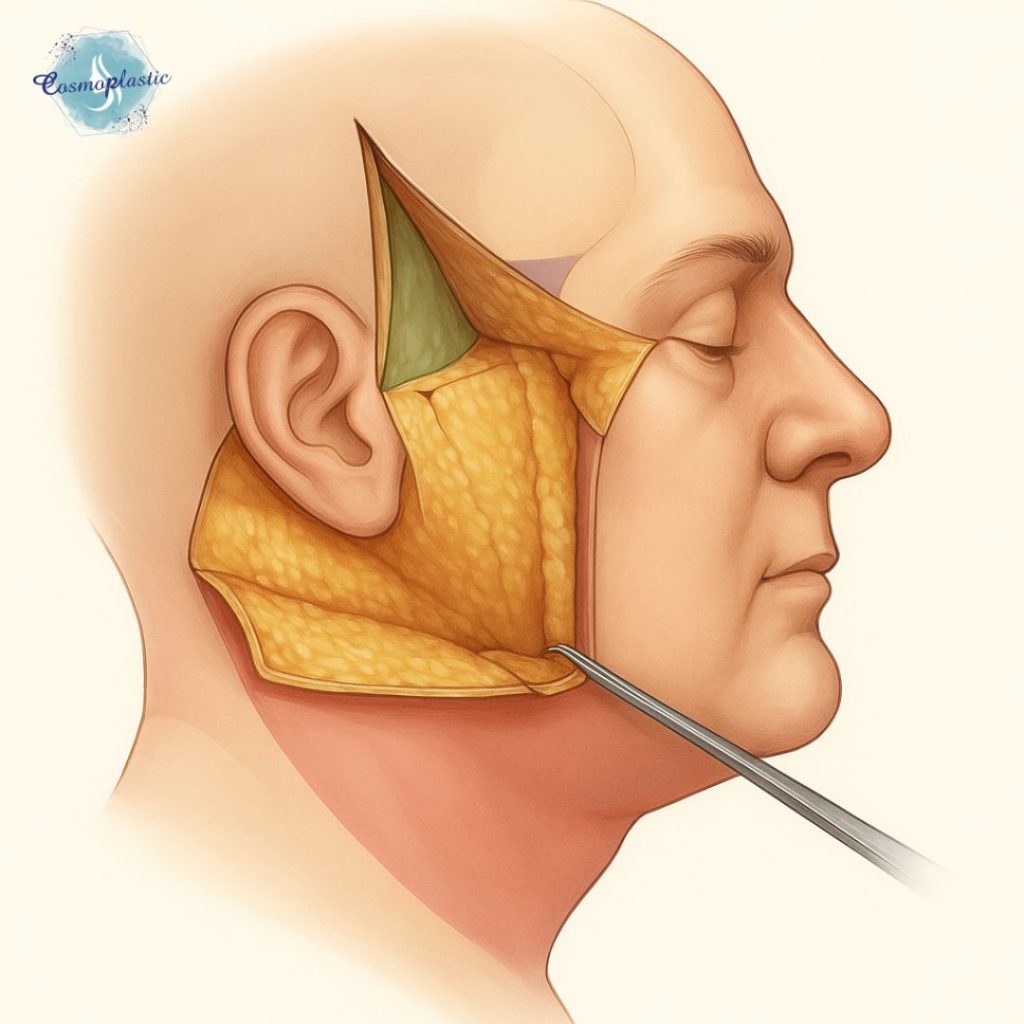
● SMAS Flap Elevation: Allows access to midfacial fat pads and deeper structures like the zygomaticus major and minor. It is critical for repositioning sagging facial tissues.
● Midface Volumization via Vertical Vector Lifts:
SMAS release in the deep-plane facelift enables true vertical elevation of ptotic midfacial tissues (including the malar fat pad), which is more effective for restoring youthful cheek contour compared to simple skin redraping.
● Improved Cervicomental Angle Definition:
In lower face and neck lifts, manipulation of the SMAS-platysma continuum allows for contouring the jawline and submental region, especially when combined with platysmal plication or suspension techniques.
● Perioral Rejuvenation:
Targeted SMAS dissection lateral to the oral commissure, especially near the modiolus, allows for subtle correction of marionette lines and oral commissure ptosis—though with care to avoid disrupting the facial nerve buccal branches.
● Durable Lift with Minimal Skin Tension:
Manipulating the SMAS, rather than relying solely on skin excision, allows redistribution of facial vectors while preserving natural expression and minimizing hypertrophic scars or widened incisions—critical for longevity and aesthetics.
● Rejuvenation of the Nasolabial Fold:
SMAS repositioning indirectly softens the nasolabial fold through upward redraping of malar tissues—important since direct excision of the fold is typically avoided.
● Platform for Fat Grafting or Volumization Adjuncts:
SMAS elevation exposes fat compartments and ligamentous septa, enabling targeted fat grafting or filler placement with anatomical precision—particularly in blended approaches.
● Versatility Across Techniques:
The SMAS plane serves as the anatomical foundation for hybrid techniques, such as:
- High SMAS lift (Barton technique),
- Lateral SMASectomy (Hamra),
- Composite rhytidectomy (including orbicularis oculi),
- MACS lift (Minimal Access Cranial Suspension) which anchors the SMAS using vertical sutures.
Surgical Techniques
● SMAS Plication: Folding and suturing the SMAS without excision. Faster and safer, particularly in less experienced hands.
● SMASectomy: Removal of a strip of SMAS and suturing the edges. Offers robust repositioning in experienced hands.
● Deep Plane Facelift: Involves release and elevation of the SMAS with the overlying skin as a unit, allowing repositioning of deeper midfacial fat pads for natural results.
● High SMAS Technique:
- Elevation of the SMAS flap extends superiorly over the zygomatic arch to include the malar fat pad and midface.
- This technique is particularly effective for malar flattening, tear trough hollowing, and midfacial descent, offering vertical vector lift with a natural transition.
● Extended Deep Plane Facelift:
- Involves ligamentous release of key retaining structures (e.g., zygomatic cutaneous ligament, mandibular ligaments) to achieve wider SMAS mobilization.
- Allows greater malar projection, jowl correction, and even limited periorbital rejuvenation.
● MACS Lift (Minimal Access Cranial Suspension):
- Uses short scar incision and loop sutures to elevate the SMAS in a vertical direction.
- Suitable for younger patients with early jowling, offering shorter downtime and lower morbidity, but less powerful than deep-plane lifts.
● Composite Facelift:
- Elevates the skin, SMAS, and orbicularis oculi as a single anatomical unit.
- Provides more dramatic periorbital and midface rejuvenation but is technically demanding, often reserved for advanced or revision cases.
● Sub-SMAS Undermining with SMAS Fixation Sutures:
- Used in patients with thin SMAS or in high-risk areas, where partial dissection is performed, followed by anchoring sutures to deep retaining ligaments or periosteum (e.g., mastoid, zygomatic arch).
- Blends efficacy with nerve safety.
● Lateral SMASectomy with Vector Shift:
- Involves excision of a crescent or wedge-shaped SMAS segment and redraping in an oblique or customized vector to target specific areas (e.g., marionette lines vs. jowls).
- Popularized in Hamra’s modifications.
● Hybrid SMAS Techniques:
- Combine deep plane dissection in the midface with plication or SMASectomy in the lower face.
- Maximizes benefit while limiting operative risk, tailored to facial topography and patient goals.
✏️ Quick Review Checklist
✔️ Understand the Layered Anatomy of the Face:
Always identify the skin–subcutaneous fat–SMAS–mimetic muscle–deep fascia sequence to plan safe dissection planes and optimize facelift vector design.
✔️ Know SMAS Transition Zones and Limitations:
Recognize where the SMAS becomes discontinuous or transforms (e.g., orbicularis oculi, nasalis, orbicularis oris) to avoid ineffective or risky maneuvers in areas like the eyelids, nose, and perioral region.
✔️ Respect Facial Nerve Pathways:
Critical zones include the marginal mandibular near the mandibular border, zygomatic branches near the arch, and buccal branches near the modiolus. Always stay superficial to the parotid-masseteric fascia in these regions.
✔️ Tailor Technique to Patient Anatomy and Goals:
Choose between plication, SMASectomy, deep plane, or hybrid based on tissue thickness, ptosis severity, facial fat distribution, and desired downtime versus longevity of results.
Read Next